Maternal mortality rates in pro-life vs pro-choice states
On average, maternal mortality rates (MMRs) are higher in states with abortion restrictions than states without them. This has been true since before Dobbs overturned Roe v. Wade, and remains true today.
Controlling the variables
Abortion proponents will point to this correlation and then suggest or outright claim this shows that abortion restrictions are dangerous to women’s health. But those making such claims make no attempt to account for other factors that contribute to maternal mortality.
For example, imagine you have State A and State B. State A has no limits on abortion, 10% of its population below the poverty line, and an MMR of 10 women per 100,000 live births. State B has a 6-week restriction on abortion, 20% of its population below the poverty line, and an MMR of 20 women per 100,000 live births.
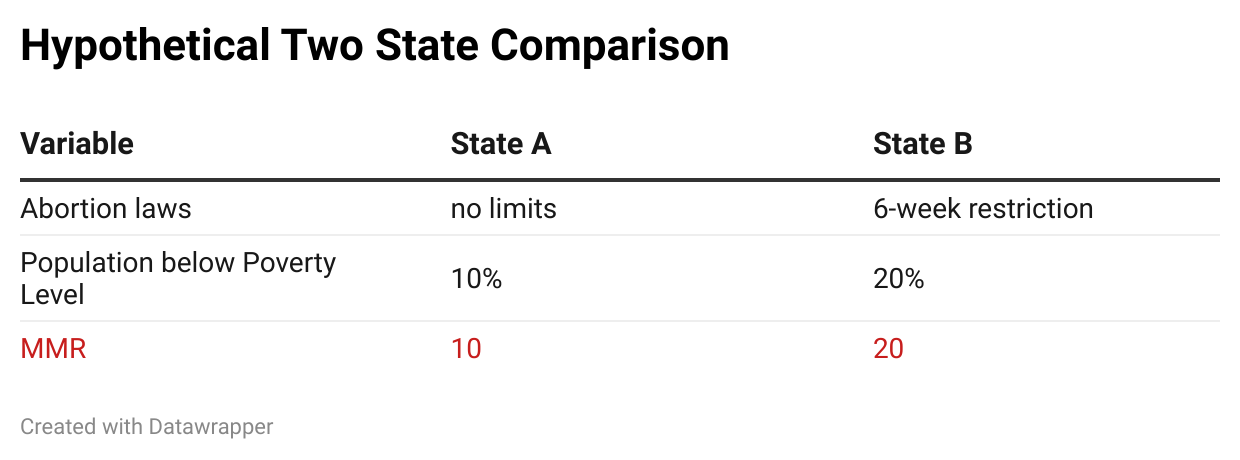
Is State B’s MMR higher because of the 6-week limit, or because twice the population is in poverty? Or both? Or neither? Without more information, we don’t know.
One way to try to get at the answer would be to compare State B to State C. State C has no limits on abortion and 20% of its population below the poverty line:
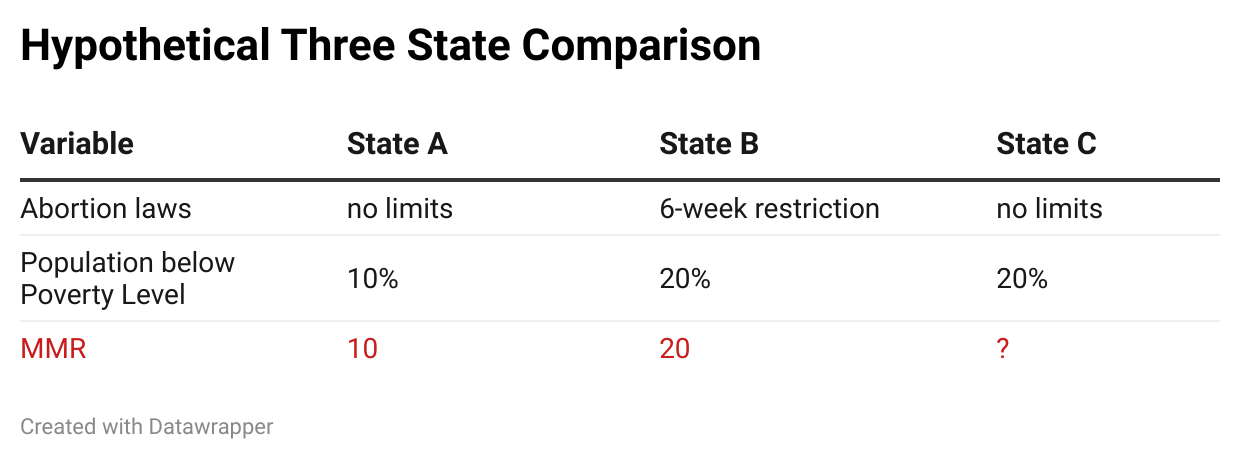
Compared to State B, will State C’s MMR be higher, lower, or the same? If State C’s MMR is higher or lower than State B’s, it may suggest abortion policy is playing a major role in MMR. If State C’s MMR is similar to State B’s, it may suggest the bigger factor here is poverty rates.
This is the kind of comparison researchers do when they’re trying to control their variables. If you want to know how abortion laws might affect MMR without the complication of different poverty levels, you compare states with similar poverty levels and different abortion laws. You’re controlling for the variable of poverty.
What factors contribute to maternal mortality rates?
I’m using poverty only as an example. There are plenty of variables that could affect MMR. Here is an incomplete list:
- Access to quality healthcare (including number of hospitals, number of OBGYNs and maternal fetal medicine specialists, midwives, doulas, birthing centers etc)
- Rural vs urban healthcare gaps
- Health insurance coverage
- Racial disparities
- Prevalence of chronic conditions (e.g. obesity, diabetes, hypertension)
- State policies regarding postpartum Medicaid coverage, maternal mental health care, and similar
- Maternal age trends
Articles like “People in states with abortion bans are twice as likely to die during pregnancy” don’t try to control for these variables. That article is referencing a Gender Equity Policy Institute (GEPI) report that starts off explaining “Even before abortion was outlawed, the states that subsequently banned abortion had worse outcomes on key indicators of reproductive health.” It does not, however, ask why. It leaves for readers to assume the only relevant factor in this discussion is state abortion policies.
[Worth noting GEPI is the same organization that claimed Texas saw a 56% increase in maternal mortality after the Texas Heartbeat Law went into effect, even though GEPI’s own numbers found no such thing. Their most recent report repeats the same falsehood. These reports are not peer-reviewed publications, which might explain why these types of claims have gone unchallenged.]
Comparing MMRs of very different states: Texas and California
The GEPI report goes on to compare Texas to California. It explains “California had the lowest maternal mortality rate of any state reporting data in 2023.” It details the different abortion policies California and Texas have enacted especially in the last few years.
But Texas already had higher MMR than California before any of the recent abortion policy changes. Remember Texas’ Heartbeat Law was enacted in September 2021, and Dobbs overturned Roe v. Wade in June 2022. But Texas has been infamous for higher MMR, and specifically compared to California, for years before these changes.
The 2018 article “Like Texas, California Once Had A Maternal Mortality Crisis. Here’s How The State Solved It” summarizes some of this. In the early 2000s California saw a spike in MMR, and so they established the California Maternal Quality Care Collaborative. For example, the Collaborative introduced “hemorrhage carts” with all the medicine and supplies doctors would need to quickly address postpartum bleeding. These kinds of initiatives helped California majorly reduce maternal mortality even as MMR was increasing nationally.
GEPI’s report frames the MMR differences between Texas and California in terms of abortion policy changes in the last few years, but (1) Texas and California have had major MMR differences for years before these abortion laws, and (2) there are major factors contributing to their different MMRs that have nothing to do with abortion policy. The GEPI report and the journalists covering it minimize or omit these kinds of considerations.
Comparing MMRs of more similar states
GEPI chose the state with the lowest MMR in the nation to represent pro-choice states and chose a state renowned for poor maternal mortality even years before Dobbs to represent pro-life ones. How do pro-choice and pro-life states compare when the states aren’t so selectively chosen?
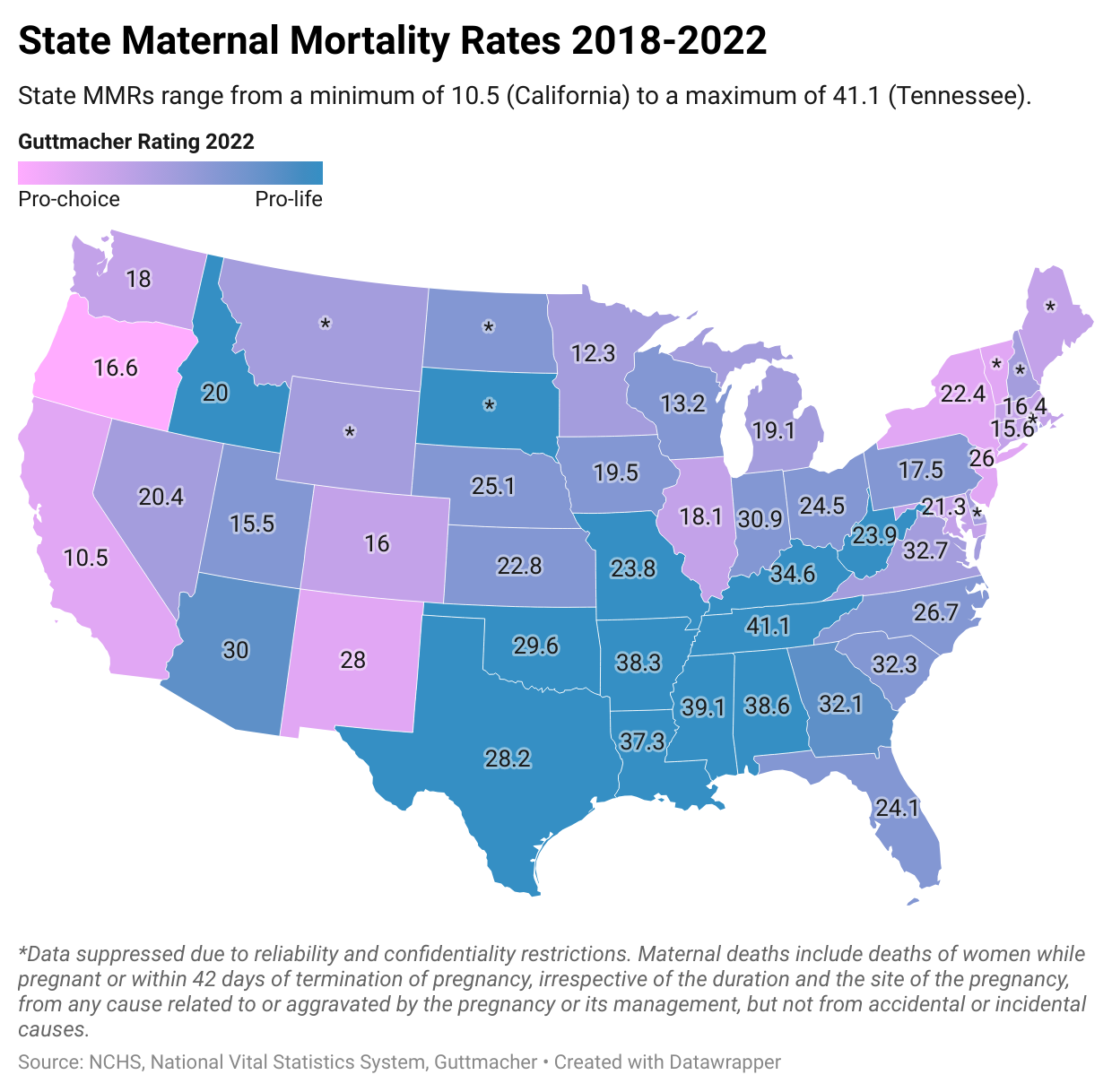
As a back-of-the-envelope look at the issue, here are comparisons of neighboring states based on MMR and abortion policy. The idea is that neighboring states may have more in common in terms of regional poverty, health status, rural vs urban environments, etc. Here’s a map of the state MMRs averaged from 2018 to 2022 according to the CDC and abortion policies for 2022 according to Guttmacher. Guttmacher rated states on a 7 point scale from most protective of abortion rights (pro-choice) to most restrictive (pro-life).
Neighboring pro-choice and pro-life states with similar MMRs
There are multiple neighboring states where one state has much more lax abortion policy than another, yet they have similar MMRs.
- Texas (MMR 28) vs New Mexico (MMR 28) In 2022, Guttmacher rated Texas “most restrictive” and New Mexico “very protective.” The Texas Heartbeat Act, which prohibits abortion after a fetal heartbeat can be detected, went into effect on September 2021, and before this, the state had many restrictions on abortion, including parental consent and a prohibition on Medicaid coverage. New Mexico has no restrictions on abortion (including no gestational limit) and is considered abortion friendly.
- Missouri (MMR 24) vs Kansas (MMR 23) Guttmacher rated Missouri “most restrictive” and Kansas “restrictive.” Missouri had many restrictions on abortion, and for most of this period, there was only one abortion clinic operating in the state. A law prohibiting abortion, with limited exceptions, went into effect in Missouri in June 2022. Kansas’s laws are less restrictive, and the state has several abortion clinics.
- Idaho (MMR 20) vs Nevada (MMR 20) Guttmacher rated Idaho “most restrictive” and Nevada “some protections.” Idaho has many restrictions on abortion, including parental consent and a prohibition on Medicaid coverage. A law prohibiting abortion, with limited exceptions, went into effect in Idaho in August 2022. Nevada has few restrictions and many abortion clinics (mostly located in Las Vegas).
- Utah (MMR 16) vs Colorado (MMR 16) Guttmacher rated Utah “restrictive” and Colorado “protective.” Utah has many restrictions on abortion, including parental consent and a prohibition on Medicaid coverage. Colorado has no restrictions on abortion (including no gestational limit) and is considered abortion friendly.
- Wisconsin (MMR 13) vs Minnesota (MMR 12) Guttmacher rated Wisconsin “restrictive” and Minnesota “some protections.” Wisconsin has some restrictions on abortion, including parental consent and a prohibition on Medicaid coverage. Minnesota has no restrictions on abortion (including no gestational limit) and is considered abortion friendly.
Neighboring pro-choice and pro-life states with higher MMRs in pro-choice states
- West Virginia (MMR 24) and Virginia (MMR 33) Guttmacher rated West Virginia “most restrictive” and Virginia “some protections.” West Virginia had banned abortion with limited exceptions and, prior to that, had required a waiting period, required physicians to provide abortions, and banned use of telehealth to mail abortion pills. Virginia didn’t limit abortion until the 3rd trimester and allowed a variety of health care professionals (not solely physicians) to provide abortions, and allowed telehealth abortions.
- Pennsylvania (MMR 18) vs New Jersey (MMR 26) and New York (MMR 22) Guttmacher rated Pennsylvania “restrictive” and New Jersey and New York “very protective.” Pennsylvania has some restrictions on abortion, including parental consent and a prohibition on Medicaid coverage. New Jersey and New York have little or no restrictions on abortion (New Jersey has no gestational limit) and are considered abortion friendly. Despite this, Pennsylvania has a significantly lower MMR than New Jersey or New York.
- Wisconsin (MMR 13) vs Illinois (MMR 18) Guttmacher rated Wisconsin “restrictive” and Illinois “protective.” Wisconsin has some restrictions on abortion, including parental consent and a prohibition on Medicaid coverage. Illinois has few restrictions on abortion and is considered abortion friendly. Despite this, Wisconsin has a significantly lower MMR than Illinois.
You can also look at the above map and find pairs of neighboring states where the pro-choice state has a lower MMR than the pro-life one. For example, Missouri and Illinois, Tennessee and North Carolina, or Oklahoma and Kansas. My point in detailing all the above pairings is not that abortion policy normally makes no difference or that pro-choice states normally have higher MMRs than pro-life ones. My point is that advocates can paint many different kinds of pictures depending on which states they choose to compare, and which variables they choose to try to control for.